The retina is the thin layer of nerve tissue lining the back of the eye.
Retinal Detachment is a condition where the retina separates from the inner wall of the eye. It is an emergency eye condition that requires urgent surgery.
The retina is the thin layer of nerve tissue lining the back of the eye.
Retinal Detachment is a condition where the retina separates from the inner wall of the eye. It is an emergency eye condition that requires urgent surgery.

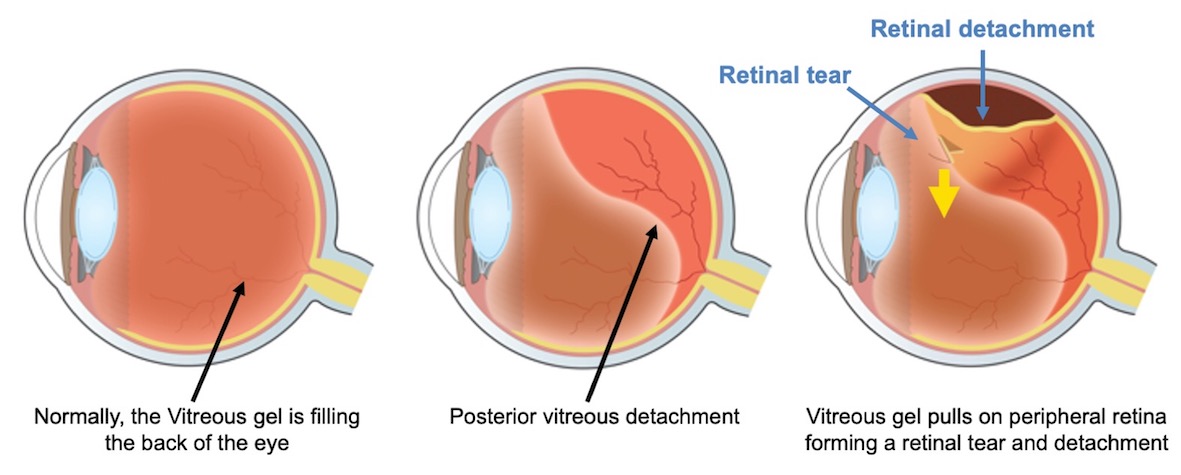
The eye is normally filled with a gel-like substance called the “vitreous”. As we age, the gel inside our eyes gradually liquifies and shrinks and may separate from the back of the eye. This process is called posterior vitreous detachment or PVD. This commonly affects people over the age of 60 years and is more common as we get older.
In a few cases of posterior vitreous detachment, the separated gel may pull on the retina leading to a retinal tear or hole. If the retinal tear is left untreated, this will allow the fluid inside the eye to pass under the retina leading to separation of the retina from the inner wall of the eye or “detachment”.
Retinal detachment itself is painless but warning signs almost always appear before it occurs or has advanced.
If you have retinal detachment, you may notice any of the following symptoms:
If untreated, this can lead to a total loss of vision as the detachment progress to involve the whole retina.
Therefore, if you notice new floaters, it’s important to have your eyes checked by a retina specialist urgently.
Retinal detachment can occur at any time with no apparent cause. It is known that some people are at a greater risk of developing retinal detachments as;
Retinal detachment is an emergency eye condition and prompt surgery is required to repair the detached retina.
The main type of surgery for retinal detachment is called “vitrectomy” which involves removing the gel inside, sealing the retinal hole or tear, and reattaching the retina to the inside of the eye. The surgery is performed with the aid of local anaesthetic (small injection of anaesthetic solution around the eye) as day surgery. Your eye will be numbed and you will not feel any pain, although you may feel some pressure sensation during the surgery. The surgery often takes about 40-60 minutes.
Vitrectomy surgery is performed by making tiny incisions, less than 1 mm, using very small instruments. First, the vitreous (gel inside the eye) is removed. Then, the retinal tear is then treated by laser or cryotherapy (a freezing treatment. The retina is repositioned in place and an internal splint is laced into the eye. This is usually a gas bubble or which supports the retina whilst healing takes place. In some situations, the surgeon may decide to put silicone oil depending upon how the eye and retina behave during the procedure. The surgery is often performed without sutures for better comfort.
Mr Ellabban will discuss with you the details of the surgery, risks and benefits, and advise you about the procedure.

In some situations, retinal detachments can be treated by another type of surgical techniques. This can be:
Scleral buckle
In this surgery, the retinal tear or hole is sealed by applying a splint to the outside wall of the eye called a “buckle”. This is stitched to the white part of the eye in the area of the retinal holes. The splint stays on the eye permanently and is not visible. It is often combined with a freezing treatment to the white of the eye to seal the retinal holes.
This type of surgery is often performed for young people (< 40 years) who develop retinal detachment. It often requires a general anaesthetic.
Pneumatic retinopexy
In this type of surgery, a small gas bubble is injected inside the eye and the retinal tear is sealed with freezing treatment. This type of surgery is often preserved to selective cases of retinal detachment.
Following the surgery, Mr Ellabban will advise if it is necessary for you to posture after surgery. If required, posturing is usually for 1-2 weeks after the surgery. The aim pf the posturing is to help the internal splint (gas or oil) to support the retina while healing takes place.

Actually, this can be the hardest part of the recovery following your surgery, but the most important. In all situations, it is important to follow the posturing instruction.
Also, if you have a gas bubble inside the eye, you will be instructed not to fly for a few weeks till the gas completely disappears.
Mr Ellabban will arrange a review after the surgery, to monitor the healing process of the retina. You will be monitored with the aid of retinal scans to assess the healing process and restoration of the retinal layers.
When the retina is successfully attached after the surgery, you will usually regain a large part of the vision. The final vision depends on whether the central part of the retina (the macula) is detached or not. It the macula is not detached; you will restore most of the vision, however, if the macula is detached, you will recover some but not all of the vision depending on the damage that may have occurred to the macula because of the detachment.
Retinal detachment surgery has similar risks as other types of eye surgery such as
Mr Ellabban will discuss with you the details of the surgery, risks and benefits in your situation, and advise you about the procedure.
You are advised to follow the instructions you were given after the surgery by Mr Ellabban and the nursing team. In general, there are important points to follow, after retinal surgery:
The success of the surgery depends on many factors like the size of the detachment, duration of the detachment and if any associated other retinal conditions. Some types of retinal detachment are more technically challenging. With modern technology, the success of retinal detachment surgery is about 85 %.
Based on the initial assessment, Mr Ellabban will be able to advise you regarding the outcome of the surgery.
Most people will need at least two weeks off work after surgery. Sometimes this may be longer. While there is gas in the eye the vision is quite poor and the ability to judge distance is affected. The amount of time off work will depend on the kind of work you do and the kind of surgery that is done. This will need to be discussed with your surgeon.
If no surgery is performed, t this usually leads to permanent loss of vision in the affected eye. Also, if the surgery is delayed, this may affect the final outcome of the surgery.
If you have been given any posturing instructions then these should be followed. You can bath or shower, but avoid splashing water near the eye. Generally you may do anything with which you are comfortable. Most people choose not to drive over the first few weeks.
If a gas bubble is used for surgery, you must not fly until the gas bubble has gone and you must inform the anaesthetist if you require a general anaesthetic for any operation while there is gas in your eye.